Important measles information for health care providers
Advisory Alert
March 21, 2024
*Cette information est seulement disponible en anglais.
To: Local Health System Partners
FOR IMMEDIATE ATTENTION
Guidance on the prevention, recognition, and reporting of measles
Given the ongoing circulation of measles virus in Ontario, Canada, and abroad, this Advisory Alert provides important information about measles prevention through immunization and will assist with the timely identification, management, and reporting of individuals who are suspected to have measles infection. All suspect cases of measles should be immediately reported to Public Health Sudbury & Districts. Do not wait for laboratory confirmation.
Immunization and disease prevention
Immunization is the best way to protect against measles infection. While it is important for everyone to be up-to-date with measles vaccine, it is especially important for individuals travelling outside of Canada. Measles-containing vaccine is part of the Ontario Publicly Funded Immunization Schedule. In Canada measles vaccines are only available as combined products and include measles-mumps-rubella (MMR) vaccines and measles-mumps-rubella-varicella (MMRV) vaccines. Product age indications differ.
Measles-containing vaccines are highly effective. The efficacy of a single dose of measles vaccine given ≥ 12 months of age is estimated to be between 85% to 95%. With a second dose, efficacy is almost 100%. Immunity following vaccination is generally lifelong.
Please review any immunization records you may have for your patients to verify that they are up-to-date with measles vaccinations in accordance with their age, current eligibility criteria, and other requirements as outlined below. For those missing vaccines, please vaccinate eligible persons as soon as possible to bring them up-to-date with current recommendations or requirements. If a patient’s immunization records are unavailable, immunization with measles-containing vaccine is recommended.
Vaccine eligibility and recommendations
The information below outlines the current recommendations for measles vaccination. Should the recommendations for measles vaccine be updated given the circulation of measles activity globally these will be shared with you immediately.
General recommendations:
| Population | Product and # of Doses | Comments |
|---|---|---|
| Infants and children as part of the routine immunization schedule • Infants ≥ 12 months of age • Children 4 to 6 years of age | 2 doses • Dose 1: MMR • Dose 2: MMRV | MMRV may be used in children from 4 to 12 years of age Recommended interval between doses: • MMR and MMR: 1 month • MMR and MMRV: 3 months MMR or MMRV vaccines must be given on the same day as other live vaccines or separated by appropriate intervals. Measles is a required vaccine under the Immunization of School Pupils Act (ISPA) and is required for attendance at licensed child care settings. |
| Unimmunized/under-immunized children and adolescents | 2 doses MMR* | *MMRV may be used in children from 4 to 12 years of age See comments above. |
| Susceptible adults born in or after 1970 | 1 dose MMR | Adults born after 1970 maybe under-immunized having received only one dose in childhood. Please consider providing a second dose of MMR vaccine based on your clinical judgment. Refer to the special populations below who require 2 doses. Please note that in the course of measles contact management, any individual born in or after 1970 who has been exposed to a measles case and has only received one dose of MMR vaccine will be considered “susceptible” and will be recommended to receive a second dose of MMR vaccine as post-exposure prophylaxis within 72 hours of exposure. |
| Adults born before 1970 | Consider 1 dose MMR 2 doses are required for select populations | Although most adults born before 1970 are considered immune from measles, some individuals may be susceptible and may be vaccinated based on a health care provider’s judgement. There are special populations in this age group (outlined below) who require immunization. |
| Special populations: regardless of year of birth, adults ≥ 26 years of age who are: • health care workers • post-secondary students • under-immunized based on a health care provider’s clinical judgement | 2 doses MMR | For these groups, the second dose of MMR vaccine is recommended. It must be given at least 4 weeks after previous MMR vaccine and separated from other live vaccines at appropriate intervals. See recommendations for health care settings below for further information. |
Recommendations for measles vaccine for travel outside of Canada:
| Population | Vaccine Product and Number of Doses | Comments |
|---|---|---|
| Infants 6 to 11 months | 1 dose MMR | 2 additional doses are required at ≥ 12 months of age at appropriate intervals and using appropriate products for age. |
| Children under 4 years of age who have received one previous dose according to the routine schedule (i.e. on or after 12 months of age) | 1 dose to complete the series | Administer the second dose of measles-containing vaccine. Product indication is based on age. |
| Individuals born in/after 1970 and those 12 months of age and older | 2 doses MMR | A 2-dose series is considered complete. Individuals with a history 1 previous dose those that are unimmunized should receive 2 doses of measles-containing vaccine in total. |
| Adults born before 1970 | 1 dose MMR | Unless there is lab evidence of immunity or history of lab-confirmed measles (see below re: serology) |
Recommendations for health care settings:
For prevention of measles transmission in health care settings, all employees (clinical and support staff) should ensure that they are immune to measles regardless of their year of birth. Proof of measles immunity includes:
- documentation of receipt of two doses of measles-containing vaccine on or after the first birthday, with doses given at least four weeks apart, or
- laboratory evidence of immunity
Vaccination is recommended over serology to determine immune status. This avoids the potential for false positive results, reduces the risk of missed opportunities for immunization and is consistent with immunization best practices as outlined in the Canadian Immunization Guide (CIG).
Clinical presentation
Please consider measles in patients presenting to you with signs and symptoms consistent with infection, particularly if they are un/under-immunized and have a potential exposure risk (recent travel, contact with a case, residency in an area with measles activity). Signs and symptoms include prodromal fever (≥ 38.3◦C oral), cough, coryza, and conjunctivitis. Koplik spots (tiny blue-white dots on the buccal mucosa) may also be present during the prodromal period. Then, 3 to 7 days after the prodromal symptoms, a red maculopapular non-itchy rash starts on the face and spreads downward and lasts for 4 to 7 days. The incubation period from exposure to prodromal period averages 10 to 12 days with time of exposure to rash onset about 14 days (range 7 to 21 days). Cases are considered infectious one day before the start of prodromal period, which is usually about four days before rash onset, to 4 days after rash onset. Individuals who have received one or 2 doses of measles-containing vaccine may develop an attenuated infection with milder symptoms.
Infection prevention and control measures
If you suspect measles infection in a patient presenting to you:
- Provide the patient with a medical mask (if able to tolerate use and no contraindications).
- Promptly isolate the patient in a negative pressure room if available (if not available, place in a single patient room with the door closed). Minimize/curtail patient movement within the setting. Only health care workers with presumptive immunity should enter the room, non-immune susceptible staff may only enter the room in exceptional circumstances (i.e. no immune health care workers are available). All health care workers regardless of presumptive immunity to measles should wear a fit-tested, seal-checked N95 respirator. Additional personal protective equipment may be required based on point-of-care risk assessment.
- Obtain specimens for testing.
- Contact Public Health Sudbury & Districts immediately to report the case (do not wait for laboratory confirmation) and to receive additional guidance.
- Provide isolation guidance to the patient while results are pending.
If an office visit is planned, schedule the patient at end of day or at a time when exposure of others can be minimized. Follow the precautions noted above.
If you suspect measles infection and the patient is an outpatient or virtual appointment, contact Public Health to arrange testing at an appropriate facility with infection prevention and control measures in place. Instruct the patient to notify health care facilities prior to arrival (when possible) to allow IPAC measures to be put in place to prevent exposures.
Following the patient’s visit, the exam room door must remain closed with signage to indicate that the room is not to be used. Allow a minimum of 2 hours of time for the air to change in the room and be free of respiratory particles before using the room for other individuals (2 hours is a conservative estimate if air exchanges are not known). Conduct routine cleaning of the room and equipment once sufficient time has elapsed to ensure adequate air exchange has occurred in the room as described above.
Testing
Please ensure you have age-appropriate supplies to support the required testing (e.g. infant/pediatric urine collector). Laboratory testing is essential for all suspect cases and includes PCR in a nasopharyngeal (NP), a throat swab, and urine. Molecular assays for measles (PCR) are the preferred diagnostic test during acute stage of illness due to higher sensitivity compared to measles serology. It is recommended that serology NOT be ordered as the only test for measles diagnosis as serology has a longer lab turn-around time and can produce a false negative in the first few days of illness. Diagnostic serology includes collection of acute and convalescent whole blood or serum samples. For the most up-to-date testing information refer to Public Health Ontario’s Laboratory Test Information Index. Timing of sample collection for NP and throat swab and whole blood or serum for acute serology is within 7 days of rash onset. Urine for PCR can be collected within 14 days of rash onset. For testing beyond the recommended time periods, consult with Public Health Ontario (PHO).
Isolation of measles virus and/or NAAT (i.e. PCR) detection is strongly recommended and should be attempted on all persons suspecting of having measles so that genotyping can be conducted. This is particularly important for persons recently vaccinated with measles-containing vaccine to differentiate wild-type versus vaccine-associated measles.
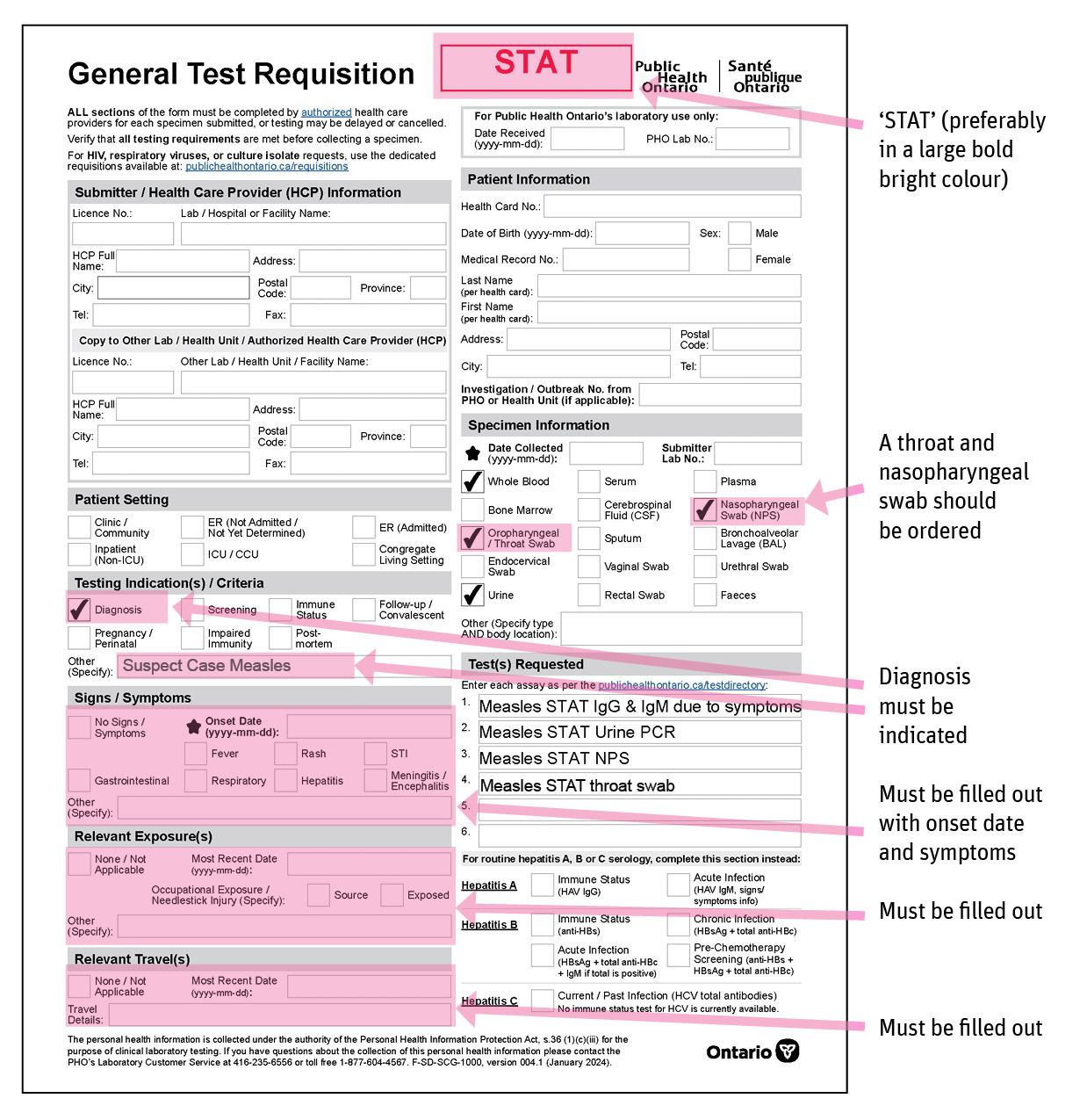
Once specimens have been collected, immediately notify Public Health Sudbury & Districts and clearly mark “suspect measles case” and STAT (bright bold letters) on each lab requisition for virus detection (PCR) and diagnostic serology. All patient demographics must be provided and ALL clinical information including symptom onset date and symptoms, exposure history, travel history (if applicable), and vaccination history must be provided. Refer to the Public Health Ontario measles webpage for further information on testing. Please see the sample requisition for measles testing located at the bottom of this Advisory Alert for your reference.
Patient counselling
Individuals with confirmed or suspected measles should be provided with the following advice to follow until the end of the infectious period. Individuals with measles are considered infectious one day before the start of prodromal period, which is usually about 4 days prior to rash onset, to 4 days after rash onset (9 days total). The onset of the rash is day 0 and is used to establish the period of communicability. Immunocompromised individuals may be infectious for longer and should be advised to isolate for the duration of illness.
- Self-isolate from all public places such as child care settings, schools, post-secondary educational institutions, work places, places of worship, sporting events, health care, and other group settings.
- Avoid contact with others not in the household.
- Avoid contact with high-risk individuals (pregnant individuals, infants < 12 months of age and immunocompromised individuals).
- Contact health care providers, hospitals, or other health care facilities prior to arrival so appropriate IPAC precautions can be implemented to avoid exposures (i.e. mask upon arrival, arrange for patient to be placed immediately in an appropriate isolation room).
- If urgent assessment is required such that they cannot call ahead, alert triage immediately of the suspect or confirmed measles diagnosis so that immediate IPAC measures can be put in place.
Contact identification and management
Public Health Sudbury & Districts will follow up with any suspected or confirmed measles case and will identify contacts and make recommendations for post-exposure prophylaxis.
Contact Public Health Sudbury & Districts
- To report an adverse event following vaccination, complete the AEFI reporting form and fax to 705.677.9616.
- To order or report a vaccine complete the Vaccine Order Form. Email to vaccineorder@phsd.caor fax to 705.677.9616. Report vaccines using the updated reporting form and fax to 705.677.9616 (the form is also available in French).
- To report a suspected or confirmed cases of measles or other disease of public health significance, call 705.522.9200, ext. 772 (toll-free 1.866.522.9200) or after hours at 705.688.4366.
- For immunization inquiries, call the Vaccine Preventable Diseases program at 705.522.9200, ext. 458 (toll-free 1.866.522.9200).
- For measles or other communicable disease inquiries call the Control of Infectious Diseases Program 705.522.9200, ext. 772 (toll-free 1.866.522.9200).
Sincerely,
Original Signed By
M. Mustafa Hirji, MD, MPH, FRCPC
Acting Medical Officer of Health and Chief Executive Officer
NOTE: All Advisory Alerts are found on our website.
This item was last modified on April 8, 2025